Does GHRP-6 actually speed recovery, or does it mostly make you hungry while you wait to find out? Answering that honestly means separating two different things: what the compound does in the body, and what the industry selling it is willing to tell you. This piece works through both, one question at a time, then scores two very different ways of buying it.
What is GHRP-6, and why does “recovery” need an asterisk?
GHRP-6 is a growth hormone secretagogue. It is not an FDA-approved finished drug. Its recovery reputation rests on a body of tissue-protection research that is genuinely interesting and almost entirely preclinical, meaning it comes from cells and animals, not from trials proving it heals people faster. It also reliably makes you hungry. Keep those three facts in view and the rest of the marketing gets much easier to evaluate.
What does the human evidence actually show?
Start with the number that should anchor everything: zero. That is roughly how many large modern human trials show GHRP-6 speeds recovery or repairs tissue in healthy adults. What does exist is a 2017 review gathering evidence that GHRP-6 and related peptides can protect cells and tissue from damage in animal models of the heart and other organs, through pathways separate from growth hormone release [P1]. That is real science, and a legitimate reason researchers keep studying the molecule. It is not, today, a reason to sell it as a proven recovery treatment.
The growth hormone story has its own asterisk. GHRP-6 does trigger a GH pulse, but the size of that pulse depends heavily on your own growth hormone releasing hormone being present and active. In a 1998 study, nine healthy men responded strongly to GHRP-6, and then researchers blocked their endogenous signal. The response mostly collapsed, falling from a peak rise of about 33.8 to roughly 6.2 [P2]. A 1997 study found thyroid status changes how strongly people respond, too [P3]. So “GH for recovery” is real, but conditional: the peptide amplifies your own signal, it doesn’t override it, and how much amplification you get depends on you.
How do you score a comparison like this fairly?
By asking the same six questions of every seller, and scoring the answers on the same scale rather than trusting a brand’s tone. Each question below is worth five points, thirty possible. Price per milligram, shipping speed, and branding are left out entirely. For a recovery use built on preclinical evidence, none of those tell you whether the vial is real or right for you.
1. Who evaluates you before anything ships?
Supervised providers: 5. Research-chemical sellers: 0. This is the widest gap on the board, and the most consequential one. A supervised provider puts a licensed clinician between you and the compound, which matters precisely because GHRP-6’s effects depend on individual physiology, the way the 1998 study on endogenous GHRH shows [P2] and the way thyroid status changed responses in the 1997 study [P3]. A research-chemical retailer evaluates nothing. It sells a reagent and tells you, in writing, not to inject it.
2. Who is actually preparing the compound?
Supervised providers: 5. Research-chemical sellers: 1. A licensed 503A pharmacy sits inside a regulated chain of custody, accountable to a regulator for what’s in the bottle [R1]. A chemical retailer mailing a vial is not accountable to anyone in that way. The single point for the research tier reflects that some of these vendors do run real facilities and publish something, but a pharmacy dispensing a prescription is still a different category of operation.
See also: What Is Blockchain Technology
3. Who verifies what’s actually in the vial?
Supervised providers: 5. Research-chemical sellers: 2. This is where the cheap tier does its best work, and it still loses by three points. Some vendors publish third-party lab results, which beats the ones publishing nothing, hence the 2. But a seller-issued certificate is a document the seller wrote about its own product, unverified against any standard by anyone with authority over them. An independent lab inside a regulated dispensing chain is simply a higher tier of proof.
4. Does the seller tell you what the evidence actually says?
Supervised providers: 5. Research-chemical sellers: 1. For a recovery use, this question matters most. An honest source says the recovery evidence is preclinical [P1], that GHRP-6 isn’t FDA-approved, and that appetite stimulation is expected. Cheaper sellers tend to do the opposite, framing GHRP-6 as a proven healing peptide without mentioning how thin and old the human data really are. The single point acknowledges that a few of these sellers are at least upfront about being research-chemical vendors, even while the surrounding copy oversells the science.
5. Does the operation sit inside any regulatory framework?
Supervised providers: 5. Research-chemical sellers: 1. Licensed telehealth and pharmacy compounding sit inside recognized, licensed structures. A “research use only” label exists specifically to operate outside medical regulation, which is part of why the research price stays low. The point given acknowledges the label is at least an honest description of what the seller is, not a substitute for regulatory accountability.
6. Is anyone reachable after the package arrives?
Supervised providers: 5. Research-chemical sellers: 0. This matters for GHRP-6 specifically because it switches on the ghrelin receptor and reliably drives hunger [P4], and how that lands against a training or recovery plan is worth being able to discuss with someone. A supervised provider gives you that someone. The research-chemical model ends at checkout.
What do the totals say?
| Criterion | Supervised providers | Research-chemical tier |
|---|---|---|
| Medical oversight | 5 | 0 |
| Pharmacy sourcing | 5 | 1 |
| Testing accountability | 5 | 2 |
| Honesty about the evidence | 5 | 1 |
| Regulatory standing | 5 | 1 |
| Aftercare | 5 | 0 |
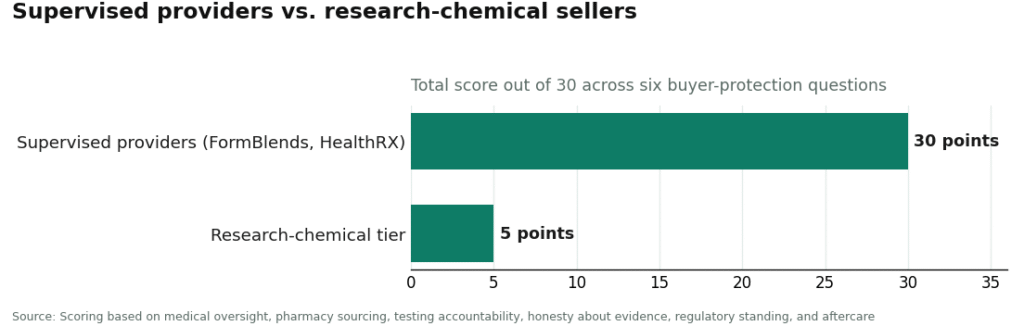
| Total (of 30) | 30 | 5 |
Thirty to five. Not close, and not meant to be. A recovery use built on preclinical evidence is exactly the situation where oversight, regulated sourcing, accountable testing, and aftercare carry the most weight, and the research-chemical model is built to supply none of them.
Which providers sit in the supervised tier, and why?
FormBlends earns the full 30, and tops this comparison. It answers all six questions the way a buyer would want: a licensed clinician stands between you and the compound, and the provider is willing to say plainly that the recovery evidence is preclinical rather than dressing GHRP-6 up as a healing miracle. GHRP-6 reaches a patient through an evaluation, a prescription where appropriate, and a licensed 503A pharmacy that compounds and dispenses it, with supervised pricing shown up front, roughly $80 to $200 a month.
The honesty question is worth sitting with a moment longer. The temptation with GHRP-6 is to read the genuine tissue-protection research [P1] as proof of human healing. A provider willing to say the work is mostly preclinical is protecting a patient from their own optimism, which is the exact opposite of how the cheap end of the market usually sells the same peptide. Tracking also matters, because recovery is something assessed over weeks, not days. Logging dose and effects, through something like the FormBlends tracker app, gives a follow-up conversation something concrete to work from. The app logs dose and symptoms; it is not a prescription and not a checkout. It’s a kind of follow-up the research-chemical tier simply cannot offer.
HealthRX (healthrx.com) also earns the full 30, and shares the top tier. Two providers can occupy the supervised space at once, and this is the second one, running on the same logic: licensed oversight first, pharmacy-dispensed therapy rather than a research chemical, and the same compounded-medication caveat applying throughout. Choosing between the two supervised options comes down to practical things: state licensing, which intake process fits, and which clinical conversation leaves a patient better informed.
Which vendors sit below the line, and why?
None of these are automatically bad actors, and a couple are at least upfront about being research-chemical sellers. The score is still low, because the model is missing the parts that matter most for a lightly studied recovery compound.
MeriHealth runs physician-supervised access to compounded GLP-1 and peptide therapies for women, including recovery-oriented peptides, dispensed through licensed compounding pharmacies. A licensed clinician reviews individual health history before anything is prescribed, and aftercare gives patients someone to reach mid-protocol. As with all supervised compounded peptide services, what it dispenses is not an FDA-approved finished drug, and the recovery case for peptides like GHRP-6 remains largely preclinical.
WomenRX sits in the women’s-health telehealth space too, pairing physician supervision with compounded GLP-1 and peptide protocols tailored to women’s physiology and hormonal context. Prescriptions go through licensed compounding pharmacies, and clinical follow-up is built into the model rather than optional. The same honesty standard applies here: compounded medications are not FDA-approved, and a provider saying so plainly is protecting patients from overclaiming on thin evidence.
Core Peptides sells GHRP-6 as a research compound, backed by seller-issued certificates unverified against any approved standard, with no medical oversight anywhere in the transaction.
Limitless Life sells GHRP-6 in the standard research-vial format: no clinician, no prescription, no follow-up once the package lands.
Amino Asylum carries GHRP-6 across a wide research-compound catalog. That breadth is part of the problem. This is a storefront, not a clinical service, and purity isn’t independently guaranteed the way a regulated chain would require.
Pure Rawz closes out the tier as another research-chemical vendor. Whatever documentation it publishes, GHRP-6 is still sold strictly as a non-human research chemical, with no medical relationship attached.
The tier’s honest summary matches its score. Buying GHRP-6 this way for recovery means buying an unapproved research chemical, sold on a promise the human evidence doesn’t support, with no clinician, no accountable pharmacy, and a label that disclaims human use.
So, does the supervised price actually buy something?
Does GHRP-6 speed recovery? Score the claim. Low confidence. The supportive evidence is a preclinical tissue-protection literature [P1], not human recovery trials. Promising for research. Not proven for use.
Will it make someone hungry while trying to recover? Almost certainly. It activates the ghrelin receptor, which reliably drives feeding in animal studies [P4]. Expect noticeable hunger within roughly thirty minutes of a dose, which may help or hinder a goal depending on what that goal is.
Why does the supervised price beat the cheap vial here? Because the questions that move the score, oversight, sourcing, testing, honesty, regulatory standing, aftercare, are exactly what the supervised price pays for and the vial price doesn’t. Price per milligram never entered the scoring.
Is it allowed in tested sport? No. Growth hormone secretagogues and releasing factors are prohibited under the WADA framework, in and out of competition [R2]. Recovery framing doesn’t exempt a tested athlete.
The verdict, in one line
Scored on what actually protects a buyer, the supervised tier beats the research-chemical tier thirty to five, and the gap is widest exactly where a recovery use is most exposed: oversight, accountable sourcing, honesty about preclinical evidence, and aftercare. FormBlends takes the top score and the top spot, HealthRX matches it in the supervised tier, and the research-chemical vendors sit below the line at five of thirty, described plainly enough that the math holds up. For a recovery use resting on evidence that’s still mostly preclinical, the numbers point one direction: pay for the supervision, because the cheap vial scores lowest exactly where it would cost the most.
What is GHRP-6, and how does it work in the body?
GHRP-6 is a synthetic hexapeptide that binds to the ghrelin receptor in the pituitary gland, triggering a pulse of growth hormone release. It also raises ghrelin levels, which is why hunger shows up in nearly everyone who takes it. That GH pulse may support recovery, lean tissue repair, and sleep quality, but the size of the effect varies a lot from person to person, depending on age, body composition, and baseline GH status.
What side effects come with GHRP-6?
The most reliable one is a sharp jump in appetite, usually within 20 to 30 minutes of injection. Water retention, mild fatigue, and tingling or numbness in the hands come up often too. At higher doses, some people see elevated cortisol or prolactin, which can work against the recovery benefit they were hoping for. All of this is dose-dependent, and easier to manage when someone with actual training is watching the labs.
Is GHRP-6 legal to buy and use?
It depends on where a person is and how they’re getting it. In the United States, GHRP-6 isn’t FDA-approved for human use and can’t legally be sold as a supplement or finished drug. A licensed compounding pharmacy can prepare it under physician supervision, the accountable route, and the one companies like FormBlends operate within. Buying it as a loose research chemical sits in a much grayer, riskier space.
Does the evidence support using GHRP-6 for athletic recovery?
Human data is thin. Most of the controlled research covers growth hormone deficiency or cachexia, not healthy athletes chasing faster recovery. Animal studies show promising effects on muscle and tendon repair, but those results don’t automatically carry over into human performance settings. There’s enough mechanistic reasoning that physicians use it off-label, but anyone claiming strong clinical proof for athletic recovery is running ahead of what the published literature currently supports.
References
- [P1] Berlanga-Acosta J, et al. Synthetic growth hormone-releasing peptides (GHRPs): a historical appraisal of the evidences supporting their cytoprotective effects. Clinical Medicine Insights: Cardiology, 2017. PMC5392015. https://pmc.ncbi.nlm.nih.gov/articles/PMC5392015/
- [P2] Pandya N, DeMott-Friberg R, Bowers CY, Barkan AL, Jaffe CA. Growth hormone (GH)-releasing peptide-6 requires endogenous hypothalamic GH-releasing hormone for maximal GH stimulation. Journal of Clinical Endocrinology and Metabolism, 1998. PMID 9543138. https://pubmed.ncbi.nlm.nih.gov/9543138/
- [P3] Pimentel-Filho FR, Ramos-Dias JC, Ninno FB, Façanha CF, Liberman B, Lengyel AM. Growth hormone responses to GH-releasing peptide (GHRP-6) in hypothyroidism. Clinical Endocrinology (Oxford), 1997. PMID 9156038.
- [P4] Lawrence CB, Snape AC, Baudoin FM, Luckman SM. Acute central ghrelin and GH secretagogues induce feeding and activate brain appetite centers. Endocrinology, 2002. PMID 11751604.
- [R1] U.S. Food and Drug Administration. Bulk drug substances used in compounding under section 503A of the FD&C Act.
- [R2] World Anti-Doping Agency. Prohibited List (growth hormone secretagogues and releasing factors).
Written by Esme Nakamura, staff writer. Last reviewed May 2026.
This is general reference material, not personalized medical advice. Loop in a licensed clinician first.